one and half year old female child was referred to us by her family doctor as he thought something wrong with her abdomen.
She was second kid born out of non consanguineous marriage ,elder one is five year old healthy boy .
No significant antenatal ,perinatal problems .
Her development was normal in all fields till ten months when she started to stand holding furniture ,from there achievement was slowed down .
Now She can walk holding on fingers which corresponding to one year.
Her manipulation ,social development corresponds to one year and three months.
In short there is mild delay in all fields , gross motor a bit more involved.
Parents took her to the family doctor when she developed running nose and fever and fever subsided in three days with symptomatic measures. Parents did not notice anything wrong with her abdomen . They were a bit concerned with the developmental delay because the elder boy achieved all the milestones earlier than her
No seizures ,no excessive irritability .
No history of any significant illness so far .
No contact with tuberculosis.
No history of travel outside .

O/E
vitals stable .
No pallor
No significant lymph nodes. No rashes, No bleeds .
GIT
Oral cavity normal
Abdomen exam showed Liver 5 cm , span 10 cm firm ,sharp margins surface smooth surface
Spleen 12 cms ,crossing the mid line. Firm .Possibility of other masses ruled out as insinuation of fingers between costal margin not possible and bi manual palpation negative .
Genitals normal
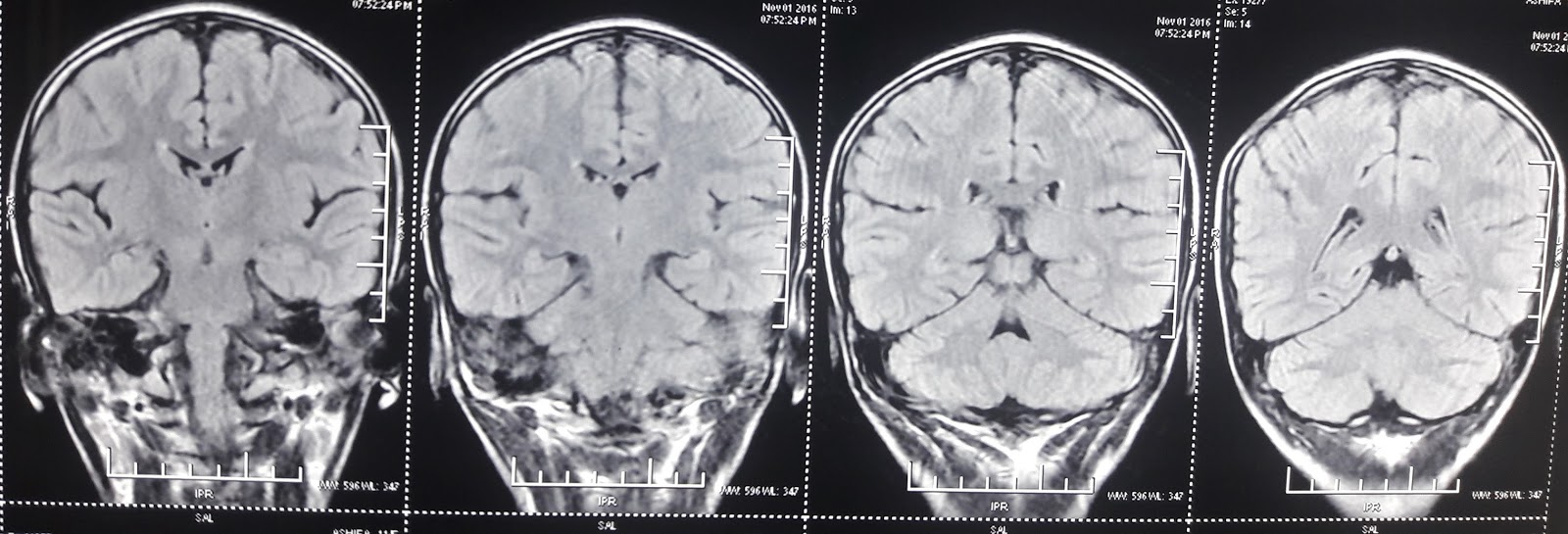
Nervous system examination
Cranial nerves all normal . Special stress on eyes. No squint ,no abnormal eye movements, Ocular movement in all directions full
( fundus normal ,no cherry red spots or optic atrophy ) ,
Discussion
In short girl child one and half years with delay in milestones , with gross spleno hepatomegaly .
Overall pattern of development she was normal up to nine months but there is slowing .Deciding about the development is one major decision
1.Is this delay significant or just a normal variation ?
2. Is it static type or Progressive type ?
A bit difficult ,because we do see mild slowing of the previous pace of development following any acute illness. So may be this is just a normal situation
But few points need to be answered before we are happy with the above argument
1. Was there a significant illness to account for this delay?
2. Of course significant illness can cause some slowing or may be a dipping of the curve , and after a gap of few week catch up . But in this case it is more than three months since they noticed the dip
3. We do get a dip or slowing following acute illness severe enough. But will it affect all the fields . Usually gross motor is the maximum affected. Here all the fields are affected .
So in short pattern of development is more like a progressive disorder . But we dont have strong evidence for it as there is nothing suggestive of a definite grey or white matter involvement so far .
Once more a rethinking
As the development is affected and a gross spleen is there bit of bias in our approach that it is a neurological problem . Did we jump to that conclusion without a second thought ?
Of course hard finding is significant spleno hepatomeglay in a young kid ? Other points are not strong enough. May be the basic entity responsible for the gross organomegaly cause bit of delay as part of its course eg a chronic infection .
So we ll take a deviant approach ignoring the development part which is not a hard finding
We ll take the dependable finding of gross spleno hepatomegaly here
What are the main entities which cause this much of organomegaly at this age ?
1. Hemolytic anemia esp thalassemia
2. Malaria
3.Malignancy ,adult type of Chronic myeloid leukemia ,rarely NHL
4.Kala Azar
5.Other hematological disorders like osteopetrosis, Myelofibrosis
She is not pale, so far no requirement of blood transfusion.
There is no fever apart from short febrile illness lasting for two days which subsided
No weight loss
These arguments argues against most of the above differentials. So this must be an entity causing significant enlargement of spleen and liver ,uniformly a bit firm in consistency ,without involving blood formation or causing blood element consumption . This is one entity not causing much of fever or inflammatory element .
Considering the above points revise the list again , excluding the above
Storage disorder
Portal hypertension
Portal hypertension without any features of liver function involvement and this huge spleen a bit unusual , not impossible .
if we give significance to development problem storage disorder is more likely.
Which one ? carbohydrate ?Lipid.? Others like Mucopolysacharide, mucolipidosis and many more .
Here no features in the general examination supporting the last groups ,
Never patient had symptoms of hypoglycemia. But glycogen storage disorder may not have symptoms ,may present with hepatomegaly only .
But spleen if at all is possible in Type 4 and it is due to portal hypertension ( reminding you , glycogen is not stored in spleen .Glycogen is stored in liver, muscles including heart , and kidneys Not in spleen . Spleen is involved in Type 4 not with storage but by portal hypertension ) This huge spleen is unlikely in portal hypertension .
Apart from this few of the general examination features which may be helpful when we consider storge of glycogen are the doll facies, and floppiness, large toungue etc. In this case none of them .
So most likely not glycogen storage.
Which one of lipid storage ? All of them can have liver and spleen enlargement . Main group are gangliosidosis 1 and 2, Spingolipidosis and cerebrosidosis
Gangliosidosis Type I look like MPS and they ll have abnormal appearance and obvious features. Type II. Tay sachs wont cause organomegally , Sandoffs organomegaly possible but small . and onset late
Neiman pick many verities are there , most of them cause predominant liver involvement . Most of them significant functional disturbance esp type C . neurological involvement esp occular , gaze etc. more prominent. Of course fundus examination ll help as all of them may have cherry red spots . But it is not a must in early stages.
Here none of the above descriptions fit with the clinical feature.
So what is remaining is Gauchers , adult type.
Out of the two types. infantile type ( adult does nt mean it ll occur in older and vice versa ) will have severe neurological problems. Here except for a minimal delay neurological examination is normal
So we considered the possibility of Gauchers
So after the basic blood counts we decided to go ahead with a bone marrow examination
We personally went to pathology department to discuss the problem and we wanted them to look for
1.Leishmaniasis
2. Malarial parasite
3.Malignancy both CML , or NHL
4.Gauchers
This is the Bone marrow picture


Patient sent home this week
We are planning an enzyme assay . The firm which markets the enzyme ll do the enzyme estimation free of charge. We have contacted them , and the tools for collection of sample awaited.
One happy news ..
Till recently cost of the enzyme replacement was around fourty lakh a year and no chance for a poor family to afford this for a lifetime . Last year one family filed a case and the verdict is favoring them , to support the cost by the govt.
I reserve my comments about the court decision and the ethical issue involved .
But we ll reveal the information to this family too .