11 year old girl with developmental delay.
Born out of non consanguineous marriage without any significant family history of seizures, mental retardation ,early childhood deaths .
No antenatal insults ,delivered at term ,cried immediately after delivery ,No neonatal problems. Initial developments were normal .Mother noticed the milestones were lagging after sitting onward. Now her Gross motor development corresponds to 7 years .Fine motor corresponds to seven years. Her language, social normal . She can read and write both English and Malayalam She can subtract ,multiply and divide numbers .
Step wise analysis
There is developmental delay
Delay predominantly in Gross motor and fine motor areas. Social and language normal
Delay is of Static type.That is gradually achieving milestones ,no regression .
Hence at this stage an entity causing developmental delay in gross motor and fine motor only with a pattern of static nature considered
When she was one and half years parents noticed abnormal jerky movements mainly involving her upper limbs and neck during episodes of fever. Initially it was attributed to drugs given for the fever.This disappeared completely after the fever in the initial episodes. There was no alteration of sensorium during these episodes. They disappeared during sleep.
Initial years she did nt have many episodes of fever. At the age of four she was investigated in NIMHANS with imaging ,biochemical tests and diagnosed as cerebral palsy ,mixed
She is now eleven years going to school, In the school her performance in mathematics is very good , Reading and understanding Malayalam ,English and hind . But her writing is bad . She writes her own ideas but occasional alphabets slips of from her pen tips.
She is brought now as the mother is concerned with her day to day activities .in between the episodes of fever also She drops things from her hands frequently . She cant drink from glass ,she spills . She cant walk holding anything straight , While trying to walk with a cup of tea her facial expression changes grossly in the effort to keep cup with water in her hands .
Examination
Vitals stable ,She is thin with normal height . Head circumference normal . Hair and skin normal , No dysmorphic features. No neurocutaneous markers .
No KF ring in the eyes .
On the left eye conjunctiva shows a prominent vascular engorgement on the sclera. No significant features on the other areas .No abnormal movements during rest .She keep her neck tilted to right side most of the times.but all neck movements normal
Nervous system examination
Intelligence memory and speech normal
Cranial nerves normal . Normal vision , fundus
Motor system ,Bulk ,power normal , Spasticity bilaterally in all limbs more in the lower limbs ,no asymmetry .Deep tendon reflexes all exaggerated ,no patellar or ankle clonus. No rigidity
( When we suspect possibility of pyramidal and extrapyramidal lesions there can be a combination of spasticity and rigidity .Spasticity after the give way feeling movement is free. If there is associated rigidity this wont be the case.
Now her abnormal movements are not obvious , spills on drinking from cup
Sensations all modalities normal
No cerebellar signs
Peripheral nerves not thickened
Skull and spine normal
Other systems normal .
At present

doubtful telangiectasia on the conjuctiva.
Now her abnormal movements are not obvious , spills on drinking from cup
Sensations all modalities normal
No cerebellar signs
Peripheral nerves not thickened
Skull and spine normal
Other systems normal .
At present

doubtful telangiectasia on the conjuctiva.
In short a case of developmental delay ,static type with pyramidal signs and chorea .Most common situation is mixed CP
Two points which raises doubt here
1. No insult to developing brain during antenatal , natal postnatal and early period of brain development
2. Episodic chorea worsened by stress .
Now she is having chorea mild nature in between . Some dystonic posturing also .
In view of episodic worsening of chorea during infections we thought of investigating to rule out underlying neuro metabolic problems. Most common entity which mimics this situation is glutaric acidemia variant
One clinical point against the possibility of neurometabolic problem is the onset at one and half years and not much of progress at this age of 11 years
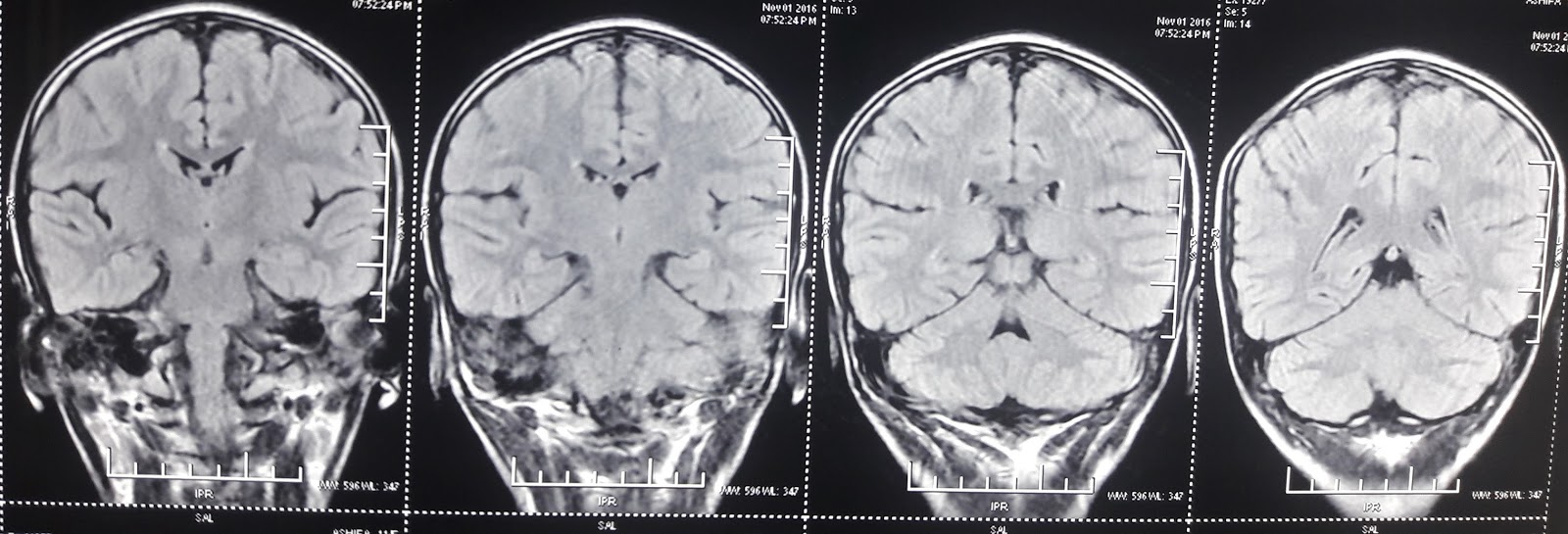
But biochemical investigation, MRI did nt support this .
So one lesson learned...Occasionally chorea in cerebral palsy may exacerbate during stress.
3/11/2016 Repeat MRI done yesterday




Two points which raises doubt here
1. No insult to developing brain during antenatal , natal postnatal and early period of brain development
2. Episodic chorea worsened by stress .
Now she is having chorea mild nature in between . Some dystonic posturing also .
In view of episodic worsening of chorea during infections we thought of investigating to rule out underlying neuro metabolic problems. Most common entity which mimics this situation is glutaric acidemia variant
One clinical point against the possibility of neurometabolic problem is the onset at one and half years and not much of progress at this age of 11 years
But biochemical investigation, MRI did nt support this .
So one lesson learned...Occasionally chorea in cerebral palsy may exacerbate during stress.
3/11/2016 Repeat MRI done yesterday







Telengiectasia was not a marker of any pathologies..?
ReplyDeleteSijith . Not sure , there is a possibility .
ReplyDelete